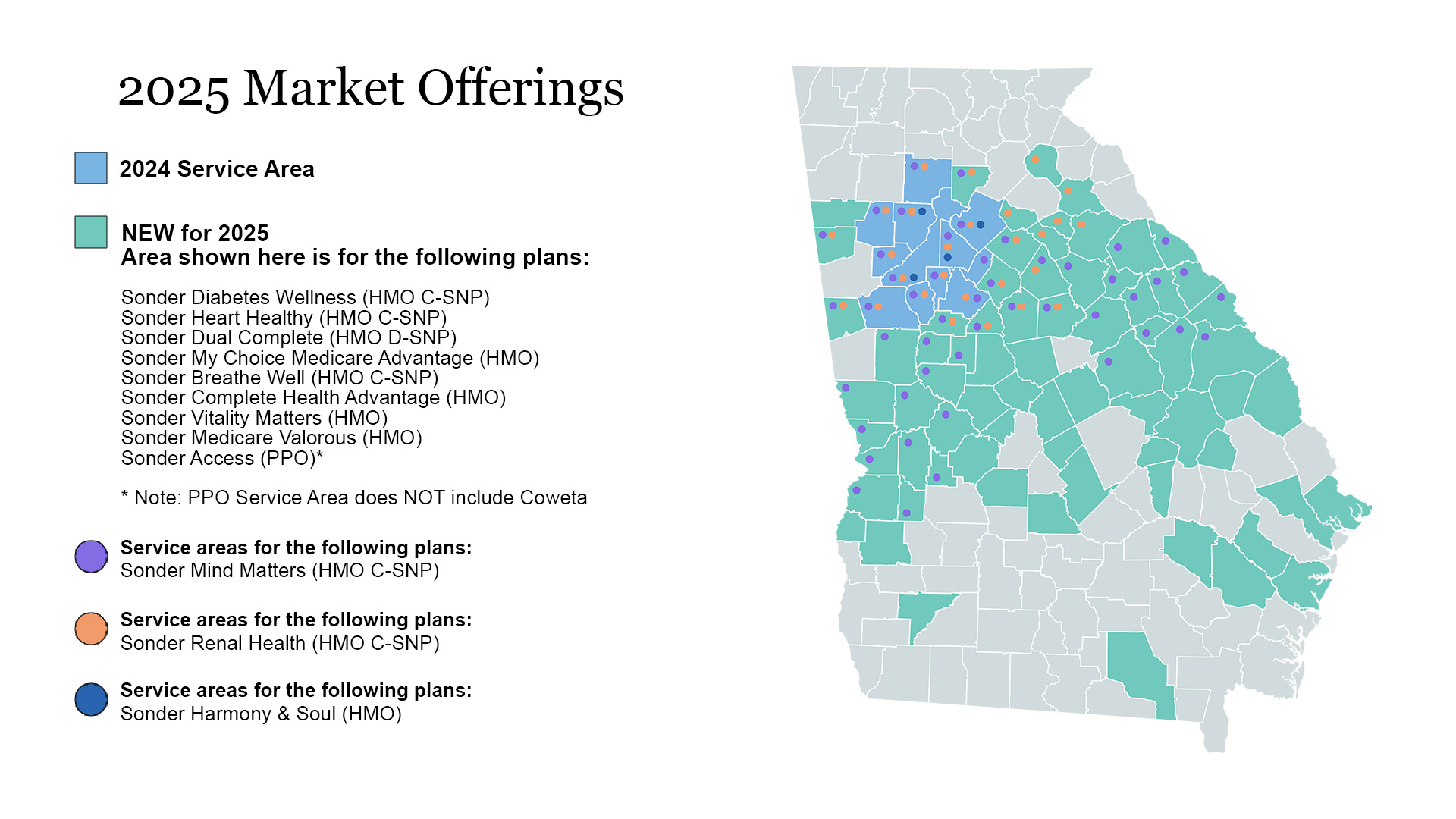
We know what you need is unique to you. Sonder Health Plans offers four plans to fit your health and lifestyle.
Explore our plans to find the right fit for you! You can see more details about each plan on the Summary of Benefits.
$0 Copay on Your PCP Visits
when you become a Sonder member
Vision, Hearing and Dental Benefits in Every Plan
$0 Copay on Your PCP Visits
when you become a Sonder Diabetes Wellness member
Vision, Hearing and Dental Benefits in Every Plan
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5; $0 days 6-90 |
| Inpatient Psych | $350 days 1-5; $0 days 6-90 |
| SNF | $0 days 1-20; $184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0 (including Intensive Cardiac Rehab and SET for PAD) |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $0.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, Dexa) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20.0% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20.0% |
| Prosthetics | 20.0% |
| Medical Supplies | 20.0% |
| Diabetic Supplies | $0.00 |
| Therapeutic Shoes or Inserts | $0.00 |
| Renal Dialysis | $0.00 |
| Chemotherapy Drugs | 20.0% |
| Part B Drugs | 20.0% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $0/$0/$0 |
| Tier 3 Insulin | $0/$0/$0 |
| Tier 4 Insulin | $0/$0/$0 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 12 one-way trips |
| OTC | $150 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $250 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Membership |
| -Internet / Cell Data |
| -Sports License (hunting/fishing) |
| -Pet Supplies |
| Members also get: |
| -$130 Grocery Card |
| -Meals: Routine – 10 per month |
| -50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 104 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depending on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0.00 |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $40.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | 20% |
| Therapeutic Shoes or Inserts | 20% |
| Renal Dialysis | 20% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $15/$45/$0 |
| Tier 3 Insulin | $35/$70/$70 |
| Tier 4 Insulin | $35/$70/$70 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 12 one-way trips |
| OTC | $200 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $325 / Month to apply towards list below (amount does NOT roll over): |
| -Adult Day Care |
| -Home Safety/Access Modifications |
| -Internet / Cell Data |
| -Pet Supplies |
| Members also get: |
| $100 Grocery Card |
| Meals: Routine – 10 per month |
| 10 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 208 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $200 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $1000 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $1000 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depeding on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0 (including Intensive Cardiac Rehab and SET for PAD) |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $0.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | $0.00 |
| Therapeutic Shoes or Inserts | $0.00 |
| Renal Dialysis | 0% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $0/$0/$0 |
| Tier 3 Insulin | $0/$0/$0 |
| Tier 4 Insulin | $0/$0/$0 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | Unlimited one-way trips |
| OTC | $200 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $240 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Membership |
| -Internet / Cell Data |
| -Pet Supplies |
| Members also get: |
| $200 Grocery Card |
| Meals: Routine – 10 per month |
| 50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 208 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depending on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $20 (including Intensive Cardiac Rehab and SET for PAD), $0 for Pulmonary rehab |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $40.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20%, oxygen at 0% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | 20% |
| Therapeutic Shoes or Inserts | 20% |
| Renal Dialysis | 20% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $15/$45/$0 |
| Tier 3 Insulin | $35/$70/$70 |
| Tier 4 Insulin | $35/$70/$70 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 50 one-way trips |
| OTC | $200 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $260 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Memberships |
| -Internet / Cell Data |
| -Pet Supplies |
| Members also get: |
| $200 Grocery Card |
| Meals: Routine – 10 per month |
| 50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 104 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| 12 visit Comprehensive Smoking Cessation Program |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depeding on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0 (including Intensive Cardiac Rehab and SET for PAD) |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $40.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | $0.00 |
| Therapeutic Shoes or Inserts | $0.00 |
| Renal Dialysis | 20% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $15/$45/$0 |
| Tier 3 Insulin | $35/$70/$70 |
| Tier 4 Insulin | $35/$70/$70 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 12 one-way trips |
| OTC | $150 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $250 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Membership |
| -Internet / Cell Data |
| -Sports License (hunting/fishing) |
| -Pet Supplies* |
| Members also get: |
| -$130 Grocery Card |
| -Meals: Routine – 10 per month |
| -50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 104 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depeding on device |
 (HMO C-SNP)
(HMO C-SNP) (HMO C-SNP)
(HMO C-SNP) (HMO C-SNP)
(HMO C-SNP)Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5; $0 days 6-90 |
| Inpatient Psych | $350 days 1-5; $0 days 6-90 |
| SNF | $0 days 1-20; $184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0 (including Intensive Cardiac Rehab and SET for PAD) |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $0.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, Dexa) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20.0% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20.0% |
| Prosthetics | 20.0% |
| Medical Supplies | 20.0% |
| Diabetic Supplies | $0.00 |
| Therapeutic Shoes or Inserts | $0.00 |
| Renal Dialysis | $0.00 |
| Chemotherapy Drugs | 20.0% |
| Part B Drugs | 20.0% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $0/$0/$0 |
| Tier 3 Insulin | $0/$0/$0 |
| Tier 4 Insulin | $0/$0/$0 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 12 one-way trips |
| OTC | $150 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $250 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Membership |
| -Internet / Cell Data |
| -Sports License (hunting/fishing) |
| -Pet Supplies |
| Members also get: |
| -$130 Grocery Card |
| -Meals: Routine – 10 per month |
| -50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 104 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depending on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0.00 |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $40.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | 20% |
| Therapeutic Shoes or Inserts | 20% |
| Renal Dialysis | 20% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $15/$45/$0 |
| Tier 3 Insulin | $35/$70/$70 |
| Tier 4 Insulin | $35/$70/$70 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 12 one-way trips |
| OTC | $200 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $325 / Month to apply towards list below (amount does NOT roll over): |
| -Adult Day Care |
| -Home Safety/Access Modifications |
| -Internet / Cell Data |
| -Pet Supplies |
| Members also get: |
| $100 Grocery Card |
| Meals: Routine – 10 per month |
| 10 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 208 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $200 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $1000 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $1000 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depeding on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0 (including Intensive Cardiac Rehab and SET for PAD) |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $0.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | $0.00 |
| Therapeutic Shoes or Inserts | $0.00 |
| Renal Dialysis | 0% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $0/$0/$0 |
| Tier 3 Insulin | $0/$0/$0 |
| Tier 4 Insulin | $0/$0/$0 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | Unlimited one-way trips |
| OTC | $200 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $240 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Membership |
| -Internet / Cell Data |
| -Pet Supplies |
| Members also get: |
| $200 Grocery Card |
| Meals: Routine – 10 per month |
| 50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 208 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depending on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $20 (including Intensive Cardiac Rehab and SET for PAD), $0 for Pulmonary rehab |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $40.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20%, oxygen at 0% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | 20% |
| Therapeutic Shoes or Inserts | 20% |
| Renal Dialysis | 20% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $15/$45/$0 |
| Tier 3 Insulin | $35/$70/$70 |
| Tier 4 Insulin | $35/$70/$70 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 50 one-way trips |
| OTC | $200 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $260 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Memberships |
| -Internet / Cell Data |
| -Pet Supplies |
| Members also get: |
| $200 Grocery Card |
| Meals: Routine – 10 per month |
| 50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 104 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| 12 visit Comprehensive Smoking Cessation Program |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depeding on device |
Unless indicated, benefits are per service or per year.
*Only for members who have qualifying chronic medical conditions.
Please see Summary of Benefits for full list of conditions.
| Deductible & Max Out-Of-Pocket |
| Deductible | $0 |
| MOOP | $3,950 |
| Part A |
| Inpatient Acute | $350 days 1-5;$0 days 6-90 |
| Inpatient Psych | $350 days 1-5;$0 days 6-90 |
| SNF | $0 days 1-20;$184 days 21-100 |
| Home Health | $10 |
| Part B |
| Cardiac & Pulmonary Rehab | $0 (including Intensive Cardiac Rehab and SET for PAD) |
| PT/OT/ST | $40.00 |
| ER | $120.00 |
| Urgent Care | $25.00 |
| PCP | $0.00 |
| Chiro | $20.00 |
| Specialist | $0.00 |
| Mental Health | $40.00 |
| Podiatry | $40.00 |
| Other Health Care Professional | $35.00 |
| Psychiatry | $40.00 |
| Outpatient Lab | $0.00 |
| X-Rays | $0.00 |
| Diagnostic Radiology | $0 for diagnostic imaging (e.g., sonagrams, ultrasounds, DEXA) – $275 for advanced imaging (e.g., CT, MRI, PET) |
| Therapeutic Radiology | 20% |
| Outpatient Hospital Services | $280.00 |
| Outpatient Hospital Observation | $350.00 |
| ASC | $180.00 |
| Outpatient Substance Abuse | $75.00 |
| Ambulance – Ground | $225.00 |
| Ambulance – Air | $450.00 |
| DME | 20% |
| Prosthetics | 20% |
| Medical Supplies | 20% |
| Diabetic Supplies | $0.00 |
| Therapeutic Shoes or Inserts | $0.00 |
| Renal Dialysis | 20% |
| Chemotherapy Drugs | 20% |
| Part B Drugs | 20% |
| Part D |
| Deductible | $0 |
| ICL | $2,000 |
| Tier 1 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Retail 30/Retail 90/Mail | $15/$45/$0 |
| Tier 3 Retail 30/Retail 90/Mail | $47/$141/$141 |
| Tier 4 Retail 30/Retail 90/Mail | $100/$300/$300 |
| Tier 5 Retail 30/Retail 90/Mail | 33%/33%/33% |
| Tier 6 Retail 30/Retail 90/Mail | $0/$0/$0 |
| Tier 2 Insulin | $15/$45/$0 |
| Tier 3 Insulin | $35/$70/$70 |
| Tier 4 Insulin | $35/$70/$70 |
| Supplemental Benefits |
| Worldwide Emergency | Up to $10,000 Maximum |
| Non-Emergency Transportation | 12 one-way trips |
| OTC | $150 per quarter |
| Meals | 2 meals a day for 14 days provided immediately following each surgery or inpatient hospitalization. Up to 4 times per year |
| Fitness | Silver & Fit |
| Nursing Hotline | Covered |
| SSBCI |
|---|
| Flex Card $250 / Month to apply towards list below (amount does NOT roll over): |
| -Gas Card |
| -Home Safety/Access Modifications |
| -Social and Active Club Membership |
| -Internet / Cell Data |
| -Sports License (hunting/fishing) |
| -Pet Supplies* |
| Members also get: |
| -$130 Grocery Card |
| -Meals: Routine – 10 per month |
| -50 non medical one way trips |
| Other (SSBCI Not required) |
|---|
| In Home Support – $0 4 hour per day, up to max 104 hours per year (including home safety assessment, caregiver, social support and medication reconciliation) |
| Personal Emergency Response System |
| Routine foot care $0 – 6 visit per year |
| Routine Chiro – $0 Copay 12 visits per year |
| Dental, Vision, Hearing Flex Card: $500 |
| Platelet Rich Plasma – 6 visits / year |
| Dental |
|---|
| Dental – Preventative |
| Annual Max Benefit Amount: $2500 combined with Comprehensive |
| Exams: 1 every 6 months |
| Prophylaxis: 1 every 6 months |
| Flouride: 1 every 6 months |
| X-Rays: 1 every 2 years |
| Dental – Comprehensive |
| Annual Max Benefit Amount: $2500 combined with Preventative |
| Non-Routine Services: Unlimited |
| Diagnostic Services: Unlimited |
| Restorative Services: Unlimited |
| Endodontics: Unlimited |
| Periodontics: Unlimited |
| Extractions: Unlimited |
| Prosthodontics, Other Oral/Maxillofacial Surgery: Unlimited |
| Vision |
|---|
| Vision – Exams: |
| Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Vision – Hardware: |
| Annual Max Benefit Amount: $200 |
| Contact Lenses |
| Eyeglasses (lenses and frames) |
| Hearing | |
|---|---|
| Hearing – Exams | Medicare Covered – $30, 1 Routine Exam / year – $0 |
| Hearing – Aids | $699 or $999 copay per hearing aid, depeding on device |
If you are a Sonder Health Plans member and have questions about your benefits, please contact the Toll-Free Sonder Member Services Center
1 (888) 428-4440
TTY/TDD 711
Monday through Friday, 8:00 a.m. to 6:00 p.m.
If you are a prospective Sonder Health Plans member and are interested in learning more about us, please call a licensed agent at
(888) 217-7110 7 days a week 8:00 a.m. to 6:00 p.m.